
Dr. Nordt brings back Orthopaedic Clinical algorithm for lower back pain
November 23, 2019
About 23 years ago, the North American Spine Society, which is a multidisciplinary spine organization nationally and the American Academy of Orthopedic Surgeons came out with an algorithm for managing lower back pain. This came out on April 26, 1996.
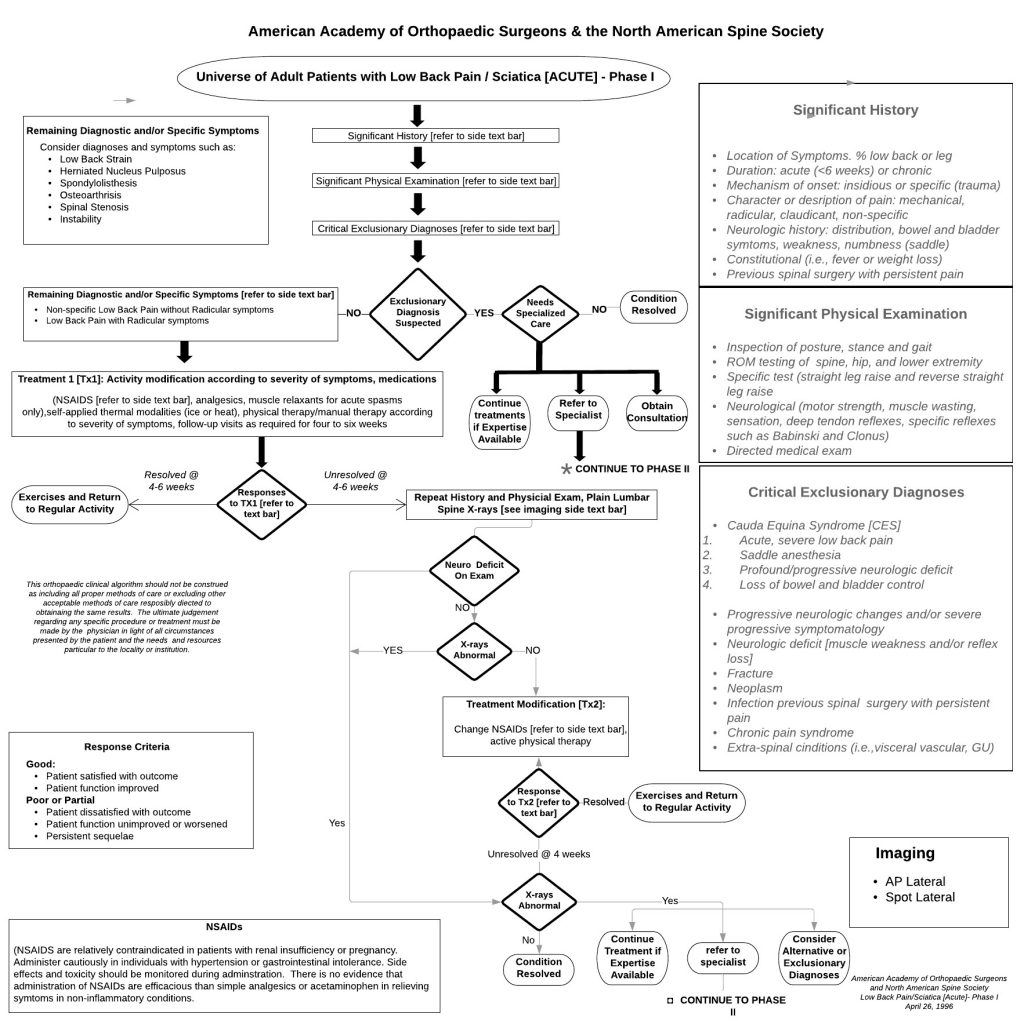
This algorithm demonstrated how to do an evaluation, and include an exclusionary diagnosis. One started off with a significant history and a full clothes off physical examination. Exclusionary diagnosis were inclusive of trauma, tumors, and previous surgeries, etc. A doctor would work through an algorithm with exercise and medication based on diagnoses. If they responded, then went back to regular activity. If not, they went to evaluating a neurological deficit with x-rays, and eventually up to four to six weeks of conservative treatment. If this failed, then that would go to Phase II of the algorithms and this is about three months later.
Phase II had to do with an update on history, physical examination, and the differential diagnosis for back pain or leg pain could be a herniated disc, instability, degenerative disc, spondylolisthesis, spinal stenosis, or some other clinical exclusionary diagnosis like a neoplasm or infection.
The algorithm continues through for herniated discs specifically, for unremitting low back pain, and whether to consider an MRI. Now be reminded, this is about two to three and even up to four to six weeks minimum before an MRI is even done. Degenerative disc, spondylolisthesis, and disc pathology can be decided whether or not that’s the pain etiology or where it’s coming from. This is also inclusive of spinal stenosis.
The point is, 23 years ago, in 1996 both the American Academy of Orthopedic Surgeons and the North American Spine Society very clearly outlined diagnostic criteria and one can follow through with these diagrams and clarify where a patient stood in the treatment plan process. There was no emphasis on pain management. It had to do with symptomatic relief with physical therapy, non-steroidal anti-inflammatory medications and steroids. Again, there is minimal narcotics mentioned on either one of these algorithms.
Should these fail, then the diagnosis may be clarified with tests? Should the diagnosis be clarified by unresolved treatment when moved on to the next plan? The next plan, Phase II was clarifying the diagnosis of the ones mentioned earlier and then determining which one of them were the correct. A specific diagnosis eventually proceeded forward with a surgical procedure.
This is where we were 25 years ago, and unfortunately people go right to an MRI, operate with some degree, or lack of degree of success.


