
The importance of proper diagnosis and treating fractures early
January 16, 2017
A 91 year old patient fell in early January and suffered from a T12 Compression Fracture. She was seen and evaluated in the Emergency Room of a well known local hospital by a neurosurgeon. The patient was told she was too old to have surgery and was subsequently ordered a special brace (TLSO or thoracolumbosacral orthosis) to manage scoliosis. She was then sent to a rehabilitation facility. She could not go to a spine fracture doctor.
This patient was on Coumadin for atrial fibrillation. She also had a pacemaker so an MRI could not be performed, and she was confined to the rehab facility for several weeks where they had her exercising and walking with poor compliance of the brace.
She was referred to me by an orthopedic surgeon in Miami and I saw her on February 10th. A bright woman who had been a hospital volunteer for 30 years, she was suffering with severe constipation and after detailed questioning, I determined that she had a severe ileus, a common finding after a compression fracture (blockage of the intestine) which was exacerbated by the blood thinner. Further, she had been given OxyContin for pain which worsened the ileus, for a 91 year old patient, is unacceptable.
I immediately admitted her to the local hospital to resolve the constipation. I spoke to her cardiologist as well as the ER physician. I ordered a bone scan because the MRI could not be done. I asked the cardiologist to lower the Coumadin and recommended a kyphoplasty procedure to treat the fracture.
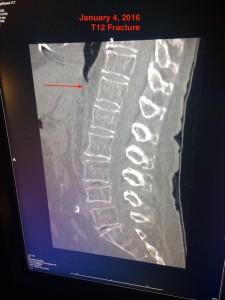
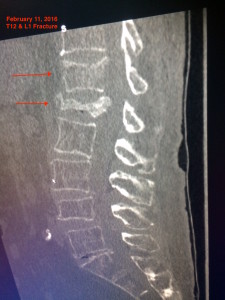
A repeat CAT SCAN showed a complete collapse of the L1 vertebrae. I compared the CAT SCAN to a month before and there was no collapse at L1. Now there were two fractures, which may have been avoided if this patient was treated early.
I ordered a Bone Scan that showed a fracture at two levels, T12 and L1 vertebrae. This was the reason she had such pain. The constipation was resolved with suitable treatment.
Her Coumadin levels dropped to the point where her INR (International Normalized Ratio) was 1. INR basically measures how long it takes for blood to clot. We performed a successful two level kyphoplasty on February 16th and the patient is now out of pain and feeling great.
I am documenting this because the patient did not have adequate medical treatment for her fracture. Oxycontin should not be prescribed for any fracture, specifically for spine because of complications. A clarification of the fracture at two levels underlines the cause for the severe constipation which was then made worse by the narcotics.
When I saw her in the office on the first day, the TLSO (back brace) she was wearing, was improperly put on. It would not support a T12 or an L1 fracture adequately. Improper or poorly supervised bracing doesn’t help. 5 weeks later she underwent a Balloon Kyphoplasty which was a reduction and stabilization of both vertebrae.
Pain relief was 100%, and this was completed under local anesthesia in under 30 minutes.

Placement of cement at T12 & L1 to stabilize the fractures after reduction with a balloon kyphoplasty
Currently, this patient is doing well, and from my perspective, that is the only goal and should be from day one. The Kyphoplasty should have been performed on days 2, 3, or latest 4 and not 6 weeks later.
It has become something of a battle cry for me but without proper diagnosis, there is no right treatment. Ever. And the patients tell us what we need to hear if we’re truly willing to listen.


